 Old Web
Old Web
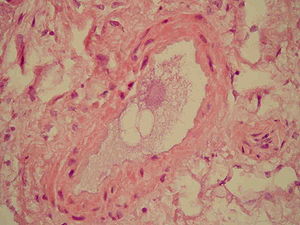
Fat embolism syndrome

Fat embolism syndrome occur when fat enters the blood stream (fat embolism) and results in symptoms. Symptoms generally begin within a day. This may include a petechial rash, decreased level of consciousness, and shortness of breath. Other symptoms may include fever and decreased urine output. The risk of death is about 10%. Fat embolism syndrome occur when fat enters the blood stream (fat embolism) and results in symptoms. Symptoms generally begin within a day. This may include a petechial rash, decreased level of consciousness, and shortness of breath. Other symptoms may include fever and decreased urine output. The risk of death is about 10%. Fat embolism most commonly occurs as a result of fractures of bones such as the femur or pelvis. Other potential causes include pancreatitis, orthopedic surgery, bone marrow transplant, and liposuction. The underlying mechanism involved widespread inflammation. Diagnosis is based on symptoms. Treatment is mostly supportive care. This may involve oxygen therapy, intravenous fluids, albumin, and mechanical ventilation. While small amounts of fat commonly occur in the blood after a bone fracture, fat embolism syndrome is rare. The condition was first diagnosed in 1862 by Zenker. Symptoms of fat embolism syndrome (FES) can start from 12 hours to 3 days after diagnosis of the underlying clinical disease. The three most characteristic features are: respiratory distress, neurological features, and skin petechiae. Respiratory distress (present in 75% of the cases) can vary from mild distress which requires supplemental oxygen to severe distress which requires mechanical ventilation. For neurologic features, those who have FES may become lethargic, restless, with a drop in glasgow coma scale (GCS) due to cerebral oedema rather than cerebral ischaemia. Therefore, neurological signs are not lateralised to one side of the body. In the severe form of cerebral odema, a person may become unresponsive. Petechiae rash usually happens in 50% of the patients. Such skin manifestation is temporary and can disappear within one day. The fat embolism syndrome can be divided into three types: Orthopaedic injuries especially fractures of the long bones are the most common cause of fat embolism syndrome (FES). The rates of fat embolism in long bone fractures varies from 1% to 30%. The mortality rate of fat-embolism syndrome is approximately 10–20%. However, fat globules have been detected in 67% of those with orthopaedic trauma and can reach as high as 95% if the blood is sampled near the fracture site. As the early operative fixation of long bone fractures become a common practice, the incidence of FES has been reduced to 0.9% to 11%. Other rare causes of fat embolism syndrome are: Once fat particles enter the blood circulation, it can lodge at various sites of the body, most commonly in the lungs (up to 75% of the cases). However, it can also enter the brain, skin, eyes, kidneys, liver, and heart circulation, causing capillary damage, and subsequently organ damage in these areas. There are two theories that describes the formation of a fat embolus: Fat embolism is presence of fat particles in the micro-circulation of the body. Meanwhile, fat embolism syndrome is the clinical manifestation as the result of fat particles lodging in the body micro-circulation. There are three major diagnostic criteria proposed for fat embolism syndrome, however, none of them are validated and accepted universally. However, Gurd and Wilson's criteria for fat embolism become more commonly used when compared to the other two diagnostic criteria. Major criteria
- CCF Conference Analysis
- Map Galaxy
- Academic Report
- What's New