 Old Web
Old Web
Defibrillation

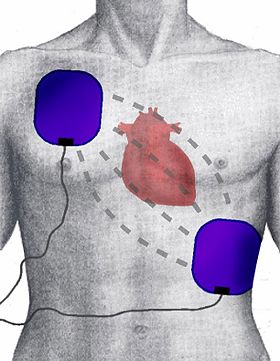
Defibrillation is a treatment for life-threatening cardiac dysrhythmias, specifically ventricular fibrillation (VF) and non-perfusing ventricular tachycardia (VT). A defibrillator delivers a dose of electric current (often called a counter-shock) to the heart. Although not fully understood, this would depolarize a large amount of the heart muscle, ending the dysrhythmia. Subsequently, the body's natural pacemaker in the sinoatrial node of the heart is able to re-establish normal sinus rhythm. Defibrillation is a treatment for life-threatening cardiac dysrhythmias, specifically ventricular fibrillation (VF) and non-perfusing ventricular tachycardia (VT). A defibrillator delivers a dose of electric current (often called a counter-shock) to the heart. Although not fully understood, this would depolarize a large amount of the heart muscle, ending the dysrhythmia. Subsequently, the body's natural pacemaker in the sinoatrial node of the heart is able to re-establish normal sinus rhythm. In contrast to defibrillation, synchronized electrical cardioversion is an electrical shock delivered in synchrony to the cardiac cycle. Although the person may still be critically ill, cardioversion normally aims to end poorly perfusing cardiac dysrhythmias, such as supraventricular tachycardia. Defibrillators can be external, transvenous, or implanted (implantable cardioverter-defibrillator), depending on the type of device used or needed. Some external units, known as automated external defibrillators (AEDs), automate the diagnosis of treatable rhythms, meaning that lay responders or bystanders are able to use them successfully with little or no training. Defibrillation is often an important step in cardiopulmonary resuscitation (CPR). CPR is an algorithm-based intervention aimed to restore cardiac and pulmonary function. Defibrillation is indicated only in certain types of cardiac dysrhythmias, specifically ventricular fibrillation (VF) and pulseless ventricular tachycardia. If the heart has completely stopped, as in asystole or pulseless electrical activity (PEA), defibrillation is not indicated. Defibrillation is also not indicated if the patient is conscious or has a pulse. Improperly given electrical shocks can cause dangerous dysrhythmias, such as ventricular fibrillation. Survival rates for out-of-hospital cardiac arrests are poor, often less than 10%. Outcome for in-hospital cardiac arrests are higher at 20%. Within the group of people presenting with cardiac arrest, the specific cardiac rhythm can significantly impact survival rates. Compared to people presenting with a non-shockable rhythm (such as asystole or PEA), people with a shockable rhythm (such as VF or pulseless ventricular tachycardia) have improved survival rates, ranging between 21-50%. Manual external defibrillators require the expertise of a healthcare professional. They are used in conjunction with an electrocardiogram, which can be separate or built-in. A healthcare provider first diagnose the cardiac rhythm and then manually determine the voltage and timing for the electrical shock. These units are primarily found in hospitals and on some ambulances. For instance, every NHS ambulance in the United Kingdom is equipped with a manual defibrillator for use by the attending paramedics and technicians. In the United States, many advanced EMTs and all paramedics are trained to recognize lethal arrhythmias and deliver appropriate electrical therapy with a manual defibrillator when appropriate. Manual internal defibrillators delivers the shock through paddles placed directly on the heart. They are mostly used in the operating room and, in rare circumstances, in the emergency room during an open heart procedure. Automated external defibrillators are designed for use by untrained or briefly trained laypersons. AEDs contain technology for analysis of heart rhythms. As a result, it does not require a trained health provider to determine whether or not a rhythm is shockable. By making these units publicly available, AEDs have improved outcomes for sudden out-of-hospital cardiac arrests. Trained health professionals have more limited use for AEDs than manual external defibrillators. Recent studies show that AEDs does not improve outcome in patients with in-hospital cardiac arrests. AEDs have set voltages and does not allow the operator to vary voltage according to need. AEDs may also delay delivery of effective CPR. For diagnosis of rhythm, AEDs often require the stopping of chest compressions and rescue breathing. For these reasons, certain bodies, such as the European Resuscitation Council, recommend using manual external defibrillators over AEDs if manual external defibrillators are readily available.
- CCF Conference Analysis
- Map Galaxy
- Academic Report
- What's New