 Old Web
Old Web
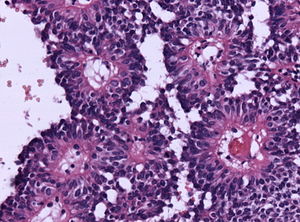
Astroblastoma

Astroblastoma is a rare glial tumor derived from the astroblast, a type of cell that closely resembles spongioblastoma and astrocytes. Astroblastoma cells are most likely found in the supratentorial region of the brain that houses the cerebrum, an area responsible for all voluntary movements in the body. It also occurs significantly in the frontal lobe, parietal lobe, and temporal lobe, areas where movement, language creation, memory perception, and environmental surroundings are expressed. These tumors can be present in major brain areas not associated with the main cerebral hemispheres, including the cerebellum, optic nerve, cauda equina, hypothalamus, and brain stem. Astroblastoma is a rare glial tumor derived from the astroblast, a type of cell that closely resembles spongioblastoma and astrocytes. Astroblastoma cells are most likely found in the supratentorial region of the brain that houses the cerebrum, an area responsible for all voluntary movements in the body. It also occurs significantly in the frontal lobe, parietal lobe, and temporal lobe, areas where movement, language creation, memory perception, and environmental surroundings are expressed. These tumors can be present in major brain areas not associated with the main cerebral hemispheres, including the cerebellum, optic nerve, cauda equina, hypothalamus, and brain stem. The most defining physical symptom of astroblastoma, regardless of location, is elevated intracranial pressure, occurring when cerebrospinal fluid in the subarachnoid space exhibits heavy pressure and decreased blood flow, resulting in throbbing headache or nausea for the patient. Despite widespread localization in the brain, astroblastoma is rarely reported in oncological studies, accounting for only 0.45–2.8% of all brain gliomas since its discovery in 1926. Without a doubt, astroblastoma remains one of the most challenging and problematic tumors to diagnose and treat among all nervous system cancers. Astroblastoma can be divided into low-grade, well-differentiated tumors and high-grade, anaplastic subtypes. The majority of tumors exhibit a spherical perimeter with either a solid or cystic interior, comprising peripheral vasculature and epithelioid neoplasms. Since the early 1890s, astroblastoma has established a stable set of pathological qualities that truly distinguishes itself as a separate and significant entity. Compilations from various case reports reveal the following common characteristics: Beyond normal pathologies, scientists have discovered some abnormal characteristics of astroblastoma in a variety of patients. The presence of a bulky calcification with punctate (pointed) and globular features was noted in a 2009 study of a 12-year-old girl. Computerized tomography confirmed these calcified masses in the posteroinferior region to the fourth ventricle just above the midline. The mass began at the brainstem, extended along the inferior cerebellar peduncle to roof areas against the ventricles through the nodule of vermis, easily detected against normal grey matter surrounding it. Calcification deriving from nervous system tumors is a rare quality in astroblastoma patients, but it is nonetheless easy to identify. Lumbar pain and lower body weakness is also a rarity in astroblastoma patients, even though it is entirely possible for lesions to proliferate toward the spinal cord. An enormous difficulty lies in classifying an astroblastoma tumor due to its overlapping features with other brain tumors. Certain neuroradiologic features finally distinguish astroblastoma from the common ependymoma, another frequent tumor occurring in the fourth ventricle. In general, when brain lesions are smaller than Grade I, demarcating between these features is near impossible, often mistaking astroblastoma with glial neoplasms, high-grade astrocytes, and embryonal neoplasms. However, the “bubbly” appearance in astroblastoma is entirely exclusive. Researchers have also confirmed astroblastoma distinct from oligodendroglioma, which are invasive nodular cysts that may resemble a 'bubbly' interior. Pleomorphic xanthoastrocytoma, dysembryoplastic neuroepithelial tumors, juvenile pilocytic astrocytoma, and hemangioblastoma are well-established, pediatric brain cancer tumors that are often confused with astroblastoma patients. However, further histology has confirmed that special structures and characteristics are unique to astroblastoma. Advances in the 21st century of histology have justified proper diagnosis, eliminating inconsistency that plagued this tumor for several decades. Research going back to early 2000 marks the first complications for satisfying requirements in radiographic and histopathologic studies. Seven astroblastoma cases of comparative genomic hybridization, a molecular technique analyzing chromosomal changes in DNA content of brain cancer cells, suggested that chromosome 19 and chromosome 20q were amplified in astroblastoma cells throughout the brain. These genomic features are responsible for widespread proliferation, tumorigenesis, and deregulation of pathways associated with normal housekeeping. Furthermore, the absence of chromosome function in 9q, 10, and X were not observed in other types of neoplasms, such as an ependymoma. Specific neuronal markers further distinguish astroblastoma. Neuron-specific enolase (NSE) positive, NSE negative, synaptophysin negative, neurofilament negative, TUJ1 positive, and nestin positive have been expressed in astroblastoma cell populations, showing significant promise in neuronal stem cell treatment for the tumor.
- CCF Conference Analysis
- Map Galaxy
- Academic Report
- What's New