 Old Web
Old Web
Polycythaemia

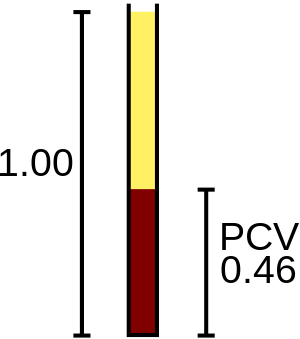
Polycythemia (also known as polycythaemia or polyglobulia) is a disease state in which the hematocrit (the volume percentage of red blood cells in the blood) is elevated. Polycythemia (also known as polycythaemia or polyglobulia) is a disease state in which the hematocrit (the volume percentage of red blood cells in the blood) is elevated. It can be due to an increase in the number of red blood cells ('absolute polycythemia') or to a decrease in the volume of plasma ('relative polycythemia'). Polycythemia is sometimes called erythrocytosis, but the terms are not synonymous, because polycythemia refers to any increase in red blood cells, whereas erythrocytosis only refers to a documented increase of red cell mass. The emergency treatment of polycythemia (e.g., in hyperviscosity or thrombosis) is by phlebotomy (removal of blood from the circulation). Depending on the underlying cause, phlebotomy may also be used on a regular basis to reduce the hematocrit. Cytostatics such as busulfan and hydroxyurea are sometimes used for long-term management of polycythemia. The overproduction of red blood cells may be due to a primary process in the bone marrow (a so-called myeloproliferative syndrome), or it may be a reaction to chronically low oxygen levels or, rarely, a malignancy. Alternatively, additional red blood cells may have been received through another process—for example, being over-transfused (either accidentally or, as blood doping, deliberately) or being the recipient twin in a pregnancy, undergoing twin-to-twin transfusion syndrome. Primary polycythemias are due to factors intrinsic to red cell precursors. Polycythemia vera (PCV), polycythemia rubra vera (PRV), or erythremia, occurs when excess red blood cells are produced as a result of an abnormality of the bone marrow. Often, excess white blood cells and platelets are also produced. PCV is classified as a myeloproliferative disease. Symptoms include headaches and vertigo, and signs on physical examination include an abnormally enlarged spleen and/or liver. In some cases, affected individuals may have associated conditions including high blood pressure or formation of blood clots. Transformation to acute leukemia is rare. Phlebotomy is the mainstay of treatment. A hallmark of polycythemia is an elevated hematocrit, with Hct > 55% seen in 83% of cases. A somatic (non-hereditary) mutation (V617F) in the JAK2 gene is found in 95% of cases, though also present in other myeloproliferative disorders. Primary familial polycythemia, also known as primary familial and congenital polycythemia (PFCP), exists as a benign hereditary condition, in contrast with the myeloproliferative changes associated with acquired PCV. In many families, PFCP is due to an autosomal dominant mutation in the EPOR erythropoietin receptor gene. PFCP can cause an increase of up to 50% in the oxygen-carrying capacity of the blood; skier Eero Mäntyranta had PFCP, which is considered to have given him a large advantage in endurance events. Secondary polycythemia is caused by either natural or artificial increases in the production of erythropoietin, hence an increased production of erythrocytes. In secondary polycythemia, 6 to 8 million and occasionally 9 million erythrocytes may occur per millimeter of blood. Secondary polycythemia resolves when the underlying cause is treated. Secondary polycythemia in which the production of erythropoietin increases appropriately is called physiologic polycythemia.
- CCF Conference Analysis
- Map Galaxy
- Academic Report
- What's New