 Old Web
Old Web
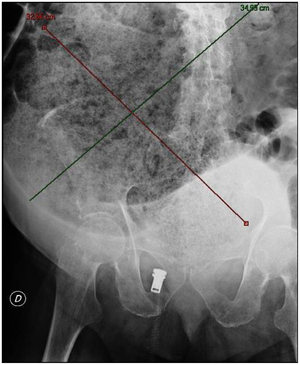
Fecal impaction

A fecal impaction is a solid, immobile bulk of feces that can develop in the rectum as a result of chronic constipation. A related term is fecal loading which refers to a large volume of stool in the rectum of any consistency. A fecal impaction is a solid, immobile bulk of feces that can develop in the rectum as a result of chronic constipation. A related term is fecal loading which refers to a large volume of stool in the rectum of any consistency. Symptoms include chronic constipation. There can be fecal incontinence and paradoxical or overflow diarrhea (encopresis) as liquid stool passes around the obstruction. Complications may include necrosis and ulcers of the rectal tissue. Abdominal pain and bloating could also be present depending on the severity of the condition. Loss of appetite can also occur. There are many possible causes; for example, physical inactivity, not eating enough (particularly of fiber), and not drinking enough water. Medications such as opioid pain relievers (suboxone, methadone, codeine, oxycodone, hydrocodone, etc.) and certain sedatives that reduce intestinal movement may cause fecal matter to become too large, hard and/or dry to expel. Specific diseases or conditions, such as irritable bowel syndrome, neurological disorders, diabetes, and autoimmune diseases such as amyloidosis, celiac disease, lupus, and scleroderma can cause constipation. Hypothyroidism can cause chronic constipation because of sluggish, slower, or weaker colon contractions. Iron supplements or increased blood calcium levels are also potential causes. Spinal cord injury is a common cause. Manual removal of a fecal impaction is often required with obese patients in traction, after a barium enema, and in poorly hydrated older adults. Reducing opiate-based medication (when possible, tolerable, and safe; prescription medication changes should be done under the supervision of a physician), and adequate intake of liquids (water) and dietary fiber and daily exercise. The treatment of fecal impaction requires both the remedy of the impaction and treatment to prevent future recurrences. Decreased motility of the colon results in dry, hard stools that in the case of fecal impaction become compacted into a large, hard mass of stool that cannot be expelled from the rectum. Various methods of treatment attempt to remove the impaction by softening the stool, lubricating the stool, or breaking it into pieces small enough for removal. Enemas and osmotic laxatives can be used to soften the stool by increasing the water content until it is soft enough to be expelled. Osmotic laxatives such as magnesium citrate work within minutes - 8 hours for onset of action, and even then they may not be sufficient to expel the stool. Osmotic laxatives can cause cramping and even severe pain as the patient's attempts to evacuate the contents of the rectum are blocked by the fecal mass. Polyethylene glycol (PEG 3350) may be used to increase the water content of the stool without cramping; however, since it may take 24 to 48 hours for it to take effect, it is not well suited to cases where the impaction needs to be removed immediately due to risk of complications or severe pain. Enemas (such as hyperosmotic saline) and suppositories (such as glycerine suppositories) work by increasing water content and stimulating peristalsis to aid in expulsion, and both work much more quickly than oral laxatives. Because enemas work in 2–15 minutes, they do not allow sufficient time for a large fecal mass to soften. Even if the enema is successful at dislodging the impacted stool, the impacted stool may remain too large to be expelled through the anal canal. Mineral oil enemas can assist by lubricating the stool for easier passage. In cases where enemas fail to remove the impaction, polyethylene glycol can be used to attempt to soften the mass over 24–48 hours, or if immediate removal of the mass is needed, manual disimpaction may be used. Manual disimpaction may be performed by lubricating the anus and using one gloved finger with a scoop-like motion to break up the fecal mass. Most often manual disimpaction is performed without general anaesthesia, although sedation may be used. In more involved procedures, general anaesthesia may be used, although the use of general anaesthesia increases the risk of damage to the anal sphincter. If all other treatments fail, surgery may be necessary.
- CCF Conference Analysis
- Map Galaxy
- Academic Report
- What's New